
Something that cannot be seen or smelt but taking even a small lick could be fatal. This article, inspired by the image for May in our 2022 PDBe calendar, focuses on the neurotoxin, botulinum toxin, the most deadly neurotoxin known to mankind. Remarkably, even with its lethality this toxin is used in cosmetic treatments, better known as BOTOX.
Bioweapon
When asked to name a poison, people may well think of cyanide but botulinum (BoNT) toxin is ~100 billion times more toxic than cyanide. It has always been on the list of top bioweapon agents, because of its extremely high toxicity and it remains a potential biowarfare threat classed as category A biological threat. Since World War II, several countries have launched bioweapons programs to develop aerosol sprays capable of delivering this deadly toxin by plane or ballistic missile and it still remains a potential bioterrorist threat to the public.
Botulism
Botulinum toxin is a neurotoxic protein, produced by strains of the anaerobic and spore forming bacterium Clostridium botulinum, which causes the disease botulism. It damages the nervous system and causes flaccid paralysis, where the muscle tone is reduced such that they cannot contract at all, along with decreased or absent tendon reflexes. On rare occasions, it can be fatal if a person does not receive prompt treatment.
Botulism poisoning is usually food-borne, either by ingesting toxin or bacterial-contaminated food, with the majority of cases caused by dairy products like fermented cheese. Intoxication also occurs from domestically fermented, canned or preserved food when the food is not prepared properly. Botulism can also occurs, although less frequently by inhalation, from Clostridium botulinum and Clostridium baratii spores which germinate inside our body and produce BoNT poisoning.
Muscle paralysis
There are seven distinct forms of botulinum neurotoxins: Types A, B , C, D, E, F and G, with new subtypes occurring frequently. All serotypes block the release of acetylcholine, the principal neurotransmitter at the neuromuscular junction, which prevents muscle contraction and eventually leads to flaccid muscle paralysis. Although all of these serotypes inhibit neurotransmitter release they differ substantially in their target proteins, characteristics of action and potencies. Typically, serotypes A, B, E and F are associated with human botulism with A, B and E being the most frequent cause of foodborne botulism. Type A is the most severe while type E has the shortest incubation period.
How does it work?
The pathology of BoNT toxicity results from intoxication of motor-neurons of the central nervous system. BoNT are large, zinc-dependent metalloproteases consisting of a 50 kDa light chain and a 100 kDa heavy chain, linked together by a single disulfide bond (Figure 1, BoNT A).

Figure 1: Crystal structure of botulinum neurotoxin type A of Clostridium botulinum . The Zn dependent metalloprotease light chain is coloured in green with Zinc shown as pink sphere, the heavy chain - translocation domain and N-terminal receptor binding domain in green and blue respectively. The catalytic zinc is depicted as a ball in pink.
The mechanism by which a BoNT intoxicates involves a 4-step process (Figure 2) -
- binding the neuronal cell receptor
- endocytosis
- membrane translocation and
- cleavage of host proteins called SNARE (Soluble N-ethylmaleimide-sensitive factor activating protein receptor) proteins.
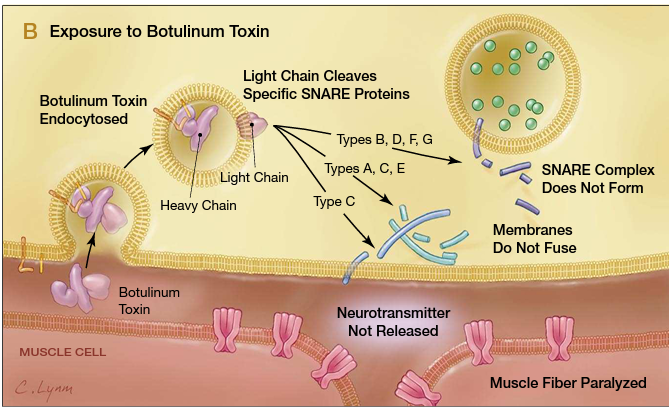
Figure 2: Schemactic representation showing the mechanism of action by botulinum neurotoxin. Image credits: JAMA. 2001;285:1059-1070 Botulinum Toxin as a Biological Weapon
The heavy chain binds the neuronal cell receptors through the C-terminal receptor binding domain (shown in Figure 3, PDB id , other structures in complex with neuronal receptor , , , ) and facilitates the translocation of light chain from the synaptic vesicle into cytosol through the N-terminal translocation domain. The change in cytoplasmic pH leads to dissociation of the light chain from the heavy chain. The light chain is the active part of the toxin that has zinc metalloprotease and it cleaves SNARE proteins (PDB id ), involved in docking and fusion of acetylcholine-containing vesicles to the postsynaptic membrane.
The cleavage of SNAREs results in the inhibition of acetylcholine release into the neuro-muscular junctions resulting in flaccid paralysis. One of the hallmarks of BoNTs, particularly serotype A is long persistence of the light chain once inside a neuron due to its lengthy half-life of several months. However, once it is ultimately degraded, inhibition of acetylcholine release resolves very rapidly.

Figure 3: Receptor binding domain of Botulinum neurotoxin A in complex with neuronal receptor, taken from . The structure is shown in cartoon format and surface representation in the background. The receptor binding domain of Botulinum neurotoxin A is shown in dark green and the neuronal receptor in light green.
BOTOX: In the name of beauty
The best wrinkle is the one that you never get! This most poisonous neurotoxin has successfully established itself as a cosmetic and therapeutic agent over the years. Among them, the well known cosmetic treatment, BOTOX® (short for Botulinum toxin), is used to make wrinkles disappear. Botox, which is made from a purified form of botulinum toxin type A, is injected into targeted areas of the face to reduce wrinkles. It works by paralysing the muscles that will relax and smooth out, thus reducing these creases or wrinkles. Due to its long lasting effect it usually lasts for around 3 or 4 months.
Wrinkle-reducing treatments that use botulinum toxin injectables may also be used to treat chronic migraines. These treatments, known as neuromodulating drugs (such as Botox, Dysport, Xeomin and Mybloc), were approved by the FDA in 2010 for migraine treatment.
It is now an accepted treatment in a wide spectrum of disorders and has over a 100 potential medical applications including treatment of numerous neuromuscular, autonomic, and sensory disorders. It was first approved in 1989 for the management of strabismus (where the eyes do not align in one direction) and blepharospasm (a rare neurological disorder with involuntary muscle contractions and spasms of the eyelid muscles).
Vaccines
Although botulism is a comparatively rare disease in humans and animals, the mortality rate can increase without instant and proper treatment. Vaccination with appropriate antigen to produce antibodies, to neutralise and clear the toxin from circulation, before it enters nerve cells. The first vaccine used to protect against botulism was a chemically detoxified extract from Clostridium botulinum. This toxoid vaccine was used to vaccinate high risk people. However, with time it lost its potency and was therefore discontinued.
The only available today for treatment of botulism is an equine-derived heptavalent antitoxin that is severely limited by adverse effects and a restricted use. More recently, heavy chain, light chain, and full-length BoNT are being utilised as candidate vaccines against botulism, with recombinant subunit vaccines in development and a bivalent vaccine in a phase II clinical trial.
Currently with limited therapies, the discovery of clinically relevant pharmacotherapeutic BoNT inhibitors or vaccines remains an urgent need for treating botulism. With time, and through further studies, it is likely that the number of conditions treated with botulinum toxin will keep expanding alongside new BoNT inhibitors or vaccines being developed.
Deepti Gupta
About the artwork
This artwork was created by Elliot Stannard, a 16 year old student from Saffron Walden County High. He chose botulinum for his artwork, as it is one of the most deadly neurotoxins in the world that has the ability to kill. Elliott describes his inspiration from the artist H.R. Giger, who brings together oil painting, supernatural gothic horror and futuristic sci-fi horror, to make a perfect match for this subject matter.
View the artwork in the .
Structures mentioned in this article
Link to all structures in PDB with BOTOX
Link to Botulinum neurotoxin type A protein at the PDBe-KB protein pages
Link to Botulinum neurotoxin type B protein at the PDBe-KB protein pages
Link to Botulinum neurotoxin type C protein at the PDBe-KB protein pages
Link to Botulinum neurotoxin type D protein at the PDBe-KB protein pages
Link to Botulinum neurotoxin type E protein at the PDBe-KB protein pages
Link to Botulinum neurotoxin type F protein at the PDBe-KB protein pages
Link to Botulinum neurotoxin type G protein at the PDBe-KB protein pages
Link to botulinum neurotoxin in complex with neuronal receptor - , , , ,
BLight chain with SNARE proteins
Sources
. Masuyer G, Davies JR, Stenmark P. International Journal of Molecular Sciences. 2021 Aug;22(15):8315. DOI: 10.3390/ijms22158315. PMID: 34361086; PMCID: PMC8346984.
Yi KH, Lee JH, Hu HW, Kim HJ. Toxins (Basel). 2022 Apr 10;14(4):268. doi: 10.3390/toxins14040268. PMID: 35448877; PMCID: PMC9032255.
. Lin L, Olson ME, Sugane T, et al. Journal of Medicinal Chemistry. 2020 Oct;63(19):11100-11120. DOI: 10.1021/acs.jmedchem.0c01006. PMID: 32886509; PMCID: PMC7581224.
. Lam KH, Tremblay JM, Perry K, et al. Plos Pathogens. 2022 Jan;18(1):e1010169. DOI: 10.1371/journal.ppat.1010169. PMID: 34990480; PMCID: PMC8769338.
. Košenina S, MartĂnez-Carranza M, Davies JR, Masuyer G, Stenmark P. Toxins. 2021 Dec;14(1):14. DOI: 10.3390/toxins14010014. PMID: 35050991; PMCID: PMC8781748.
. Shaterian N, Shaterian N, Ghanaatpisheh A, Abbasi F, Daniali S, Jahromi MJ, Sanie MS, Abdoli A. Pain Res Manag. 2022 Mar 31;2022:3284446. doi: 10.1155/2022/3284446. PMID: 35401888; PMCID: PMC8989603.
. Dressler D, Johnson EA. J Neural Transm (Vienna). 2022 Apr 9. doi: 10.1007/s00702-022-02494-5. Epub ahead of print. PMID: 35396965.
. Sundeen G1, Joseph T Barbieri. BToxins. 2017 Sep;9(9):E268. DOI: 10.3390/toxins9090268. PMID: 28869493; PMCID: PMC5618201.

